






















Teaching in Health: Utilising Pedagogy Techniques and Putting It All Together.
Introduction
Here is the second part about how to teach with pedagogy techniques with a focus on health. Part 2 demonstrates our assessment on ‘Learning How to Teach’ by using everything we had learned in Part 1. We had to showcase all our learning on teaching as my colleague and I had to prepare and present 2 lessons to a group of medical students. Each lesson would be running for 20 minutes with a topic of our choice relating to medicine. I also had to prepare and present a case study to second year medical students over a ZOOM meeting. I thoroughly enjoyed the experience and learning the pedagogy techniques, especially when Bloom’s Taxonomy was involved. Maybe one day, when I am experienced enough, I could give a whole 50-minute lecture to an entire cohort of medical students.
Part 1 ‘Teaching in Health: The How-To and Its Relevance in the Scope of Clinical Education’ is here, go ahead and have a read!
Putting it all together
Lesson 1
Below are the slides of our first tutorial/presentation session as we had to deliver the presentation in 20 minutes. We had to present as if we were presenting a lecture and incorporate everything we have learnt. This includes the background knowledge of pedagogy techniques, active and passive learning techniques, lesson plans, who is being taught, size of the group, feedback and making a rubric. In short, we had to incorporate what we have learned and teach an aspect of medicine. We chose to teach pharmacology for both lessons as we thought it was a relevant and compelling topic. Our audience: 3rd-year medical students, their age was around 20 years old, and were mostly Australians.






Reflecting on how it went
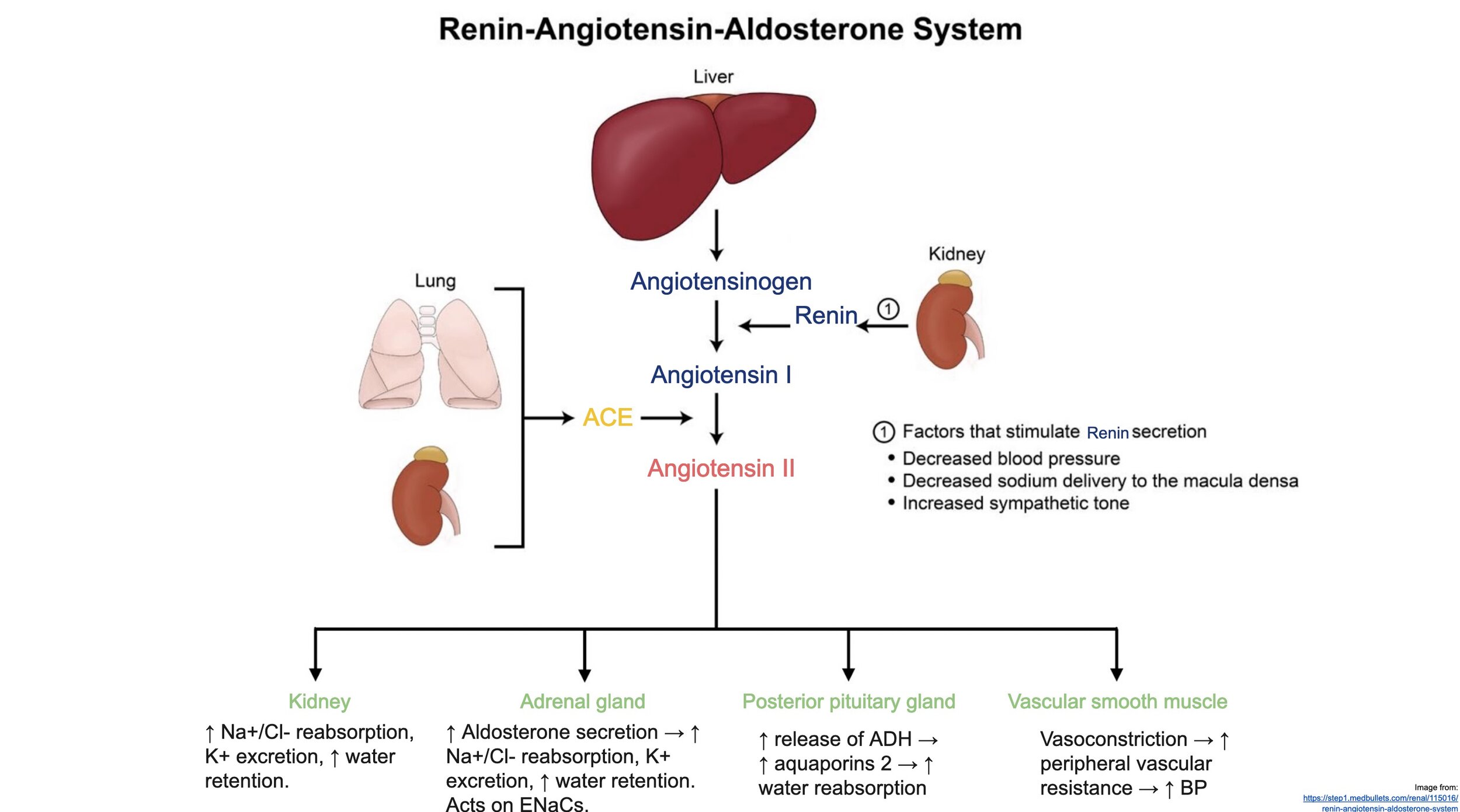
Overall, our presentation was a satisfactory first attempt in teaching health. When preparing for our presentation, we spent a significant amount of time on the topic and the learning outcomes (LO). This was critical to our presentation because it set the tone, amount of time, amount of detail we had to go in, and the reasons for teaching in the first place. We had in mind that we wanted to write about the mechanism of action (moa) of Angiotensin-Converting Enzyme (ACE) Inhibitors and Angiotensin II Receptor Blockers (ARBs). This is a difficult concept to teach as these moa(s) are involved with the Renin-Angiotensin-Aldosterone System (RAAS). The RAAS includes an intricate pathway that affects many organs around the body.
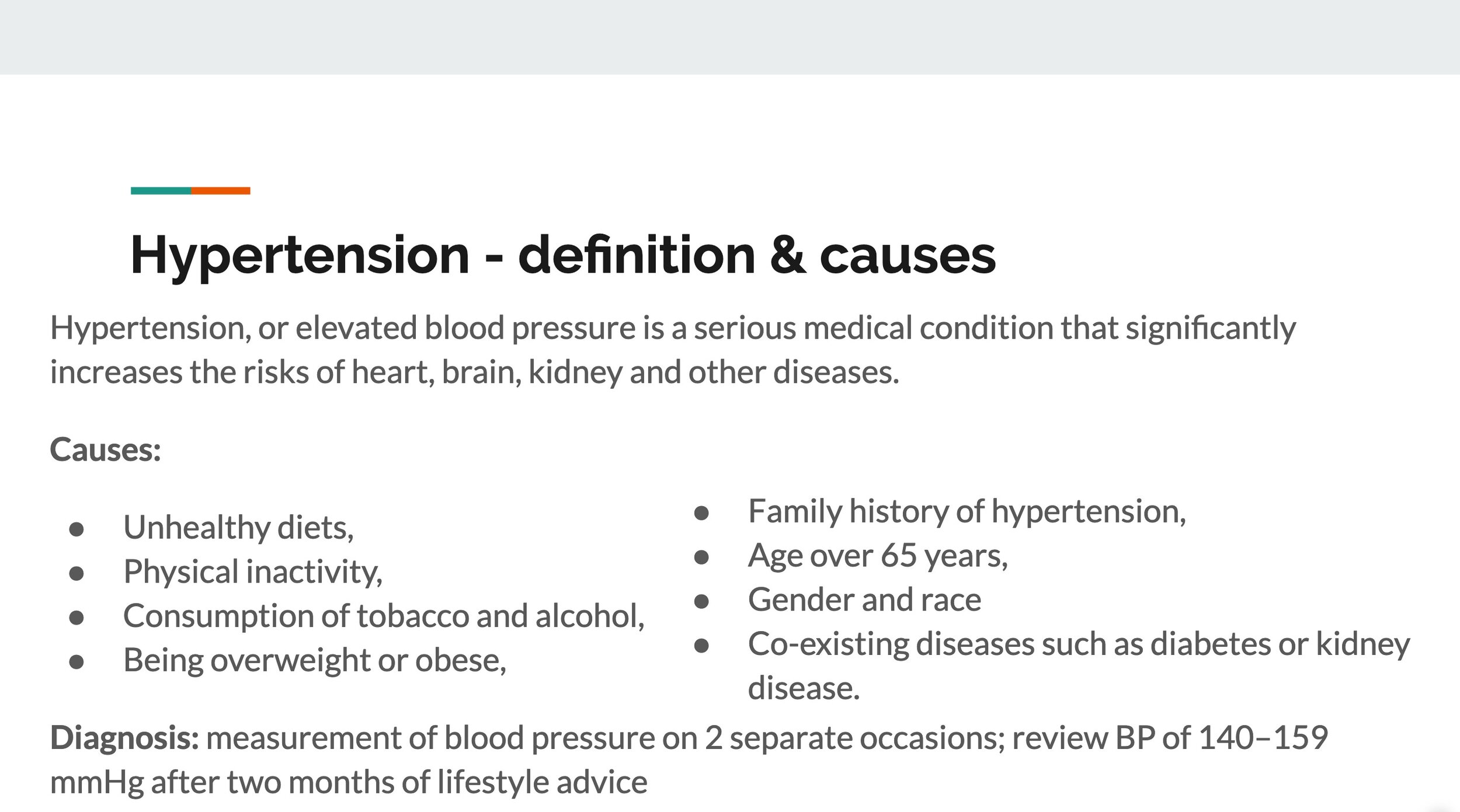
The challenge that we were facing was the amount of time and how much information should be mentioned. The amount of information given was appropriate to an audience of second-year medical students as we had covered these topics extensively. This was more of a refresher course as the students could answer with confidence our questions. We decided to relate to a common disease such as congestive heart failure or hypertension. With 1.13 billion people with hypertension (WHO), we thought it was a relevant disease to discuss.
With a sound topic chosen that contained relevant information, we started on the LO. Choosing the LO was a slight challenge; however, our primary goal was to present with three low and three high levels of LO. We settled on ‘define and list’ and ‘describe’, which represents knowledge and comprehension, respectively on Bloom’s taxonomy. For the high LO, we chose ‘compare and explain’ and ‘assess and decide’, which represented analysis and evaluation respectively on Bloom’s taxonomy. The LO reminded us to stay on track on what we were delivering. We debated on a few ideas and always related to the LO; we asked ourselves ‘do these slides answer the proposed LO?’. This was crucial as if the LO were not answered or if there were unrelated information that was given, we would have missed the target. Another critical question was: could we answer an exam with confidence if these LO were exam questions with the information given throughout this presentation?
During our presentation, we chose to use PowerPoint, fill-in missing words, human animation and a case study that was given incrementally. Due to the complexity of the moa(s) of the medications and the RAAS, we decided to incorporate a human animation that enhanced the active learning instead of using passive learning. Figure 1 below demonstrates how we decided to organize the students throughout the human animation.
Figure 1. Demonstrate how the students were being organized and helped us visualize the 3-dimensional spacing. We wanted to make sure everyone could see everything at any time.
The human animation was quite effective, and we allocated 7 minutes for this activity. The biggest challenge in our presentation was how long the students would take to act out the activity as this activity had the most unknown/uncontrollable variables. We decided I would keep a close watch on the allocated time as my colleague would do the activity. This technique was useful and would recommend it. We relied on the lesson plan, seen in Table 1 below, which helped us decide how the presentation was being organized per activity.
Table 1. Represents the lesson plan and the strategies used for each slide of the presentation.
The case study was very effective in terms of exploring the high level of Bloom’s taxonomy. The case study, given in increment as to not overwhelm the students with information, challenged the students to use all the information we have provided them and apply critically. This enabled recalling recent information given to the students and showed us if the information we had delivered was effectively applied and transferred. A case study at the end of a presentation is highly recommended as it delivers high LO and critical thinking. A case study also wraps up the presentation and enhance the points that were given throughout the presentation.
Improvements to be made is the ‘wrap-up’. It has been agreed, through the feedback we have received, that the LO shall make another appearance at the end of the presentation. We shall go through the LO and ask the students if these have been answered and if it was given in an exam how comfortable and confident they could answer. Based on the student’s feedback, we can see if the information given was appropriate and relevant. Another improvement that could be made would be preparedness. I was more nervous than I should have been and used my hands a lot, which could be improved. However, our delivery, timekeeping, professional attire and roles given from each other was done very well. We thought the presentation was smooth, relevant and effective for students to learn. We shall use all these techniques to our next presentation with the addition of LO as a final slide to recap the presentation.
Lesson 2
Here is the second lesson/presentation and we were given 20 minutes. Once again, we chose a pharmacological aspect of a particular disease and its management plan. We thought we had a successful first lesson and wanted to carry on. We kept the human animation and added a whiteboard presentation. A minor set back was that we almost run out of time.








Reflecting on how it went
Our second tutorial presentation was satisfactory with some minor improvements and a minor setback. We also decided to introduce something new to our presentation that had low risk in terms of delivery but had a relatively good yield in active learning. We decided to teach pharmacology as our first tutorial presentation on ACE-Inhibitors was quite successful. Pharmacology is a challenging and arduous, even for third-year medical students who recently have done pharmacology in their second year. Hence, we decided to deliver the best pedagogy techniques with literature background knowledge.
Nilsson et al. (2010) noted that clinical teaching is complex, which is influenced by its learning outcomes and the interactions and actions of the students. Nilsson et al. (2010) also mention that clinical teaching may be carried out in three different ways, each with a different focus either on the teacher or the student and each with their advantages and disadvantages. The pedagogy techniques were suggested initially by Ramsden (2003). These are: 1. teaching and transmission of knowledge, which is passive like, 2. organising activities for the students, which creates active learning, and 3. making the learning and understanding possible through teaching. Figure 2 below demonstrates the techniques and its focus.
Figure 2. Demonstrate the relationship between pedagogical strategies and the teachers / student focus. Suggested by Ramsden (2003).
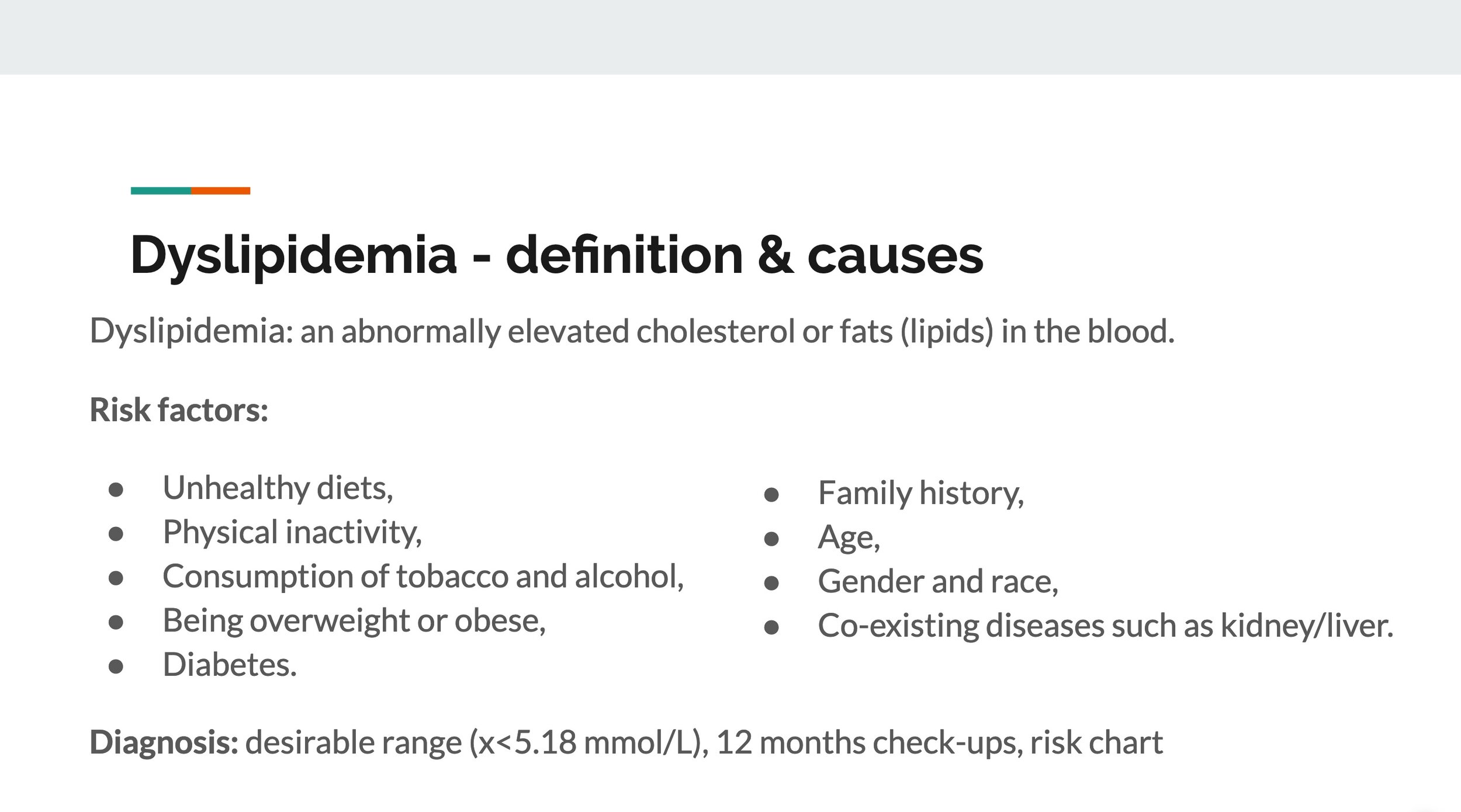
During our presentation, we implement each of these types of focus and techniques effectively by meticulously deciding where in the presentation it shall be done. Initially, we had to deliver content through lecturing. We knew this technique would be passive-like, which is not the best content delivery and retention of knowledge. When delivering a presentation, there has to be some form of passive learning. Bloom et al. (2001) demonstrate passive learning as the broadest base of Bloom’s Taxonomy Pyramid, where it is about ‘Knowledge’. This includes remembering, recalling facts or basic concepts. Hence, we realised that there was no way around this and decided to utilise this technique to its full potential by covering easy, simple and basic information. These are the types of knowledge and information that does not require a large amount of critical thinking and focus. This includes the title of the lesson, learning outcomes (LO), definitions, causes & risks, and diagnosis.
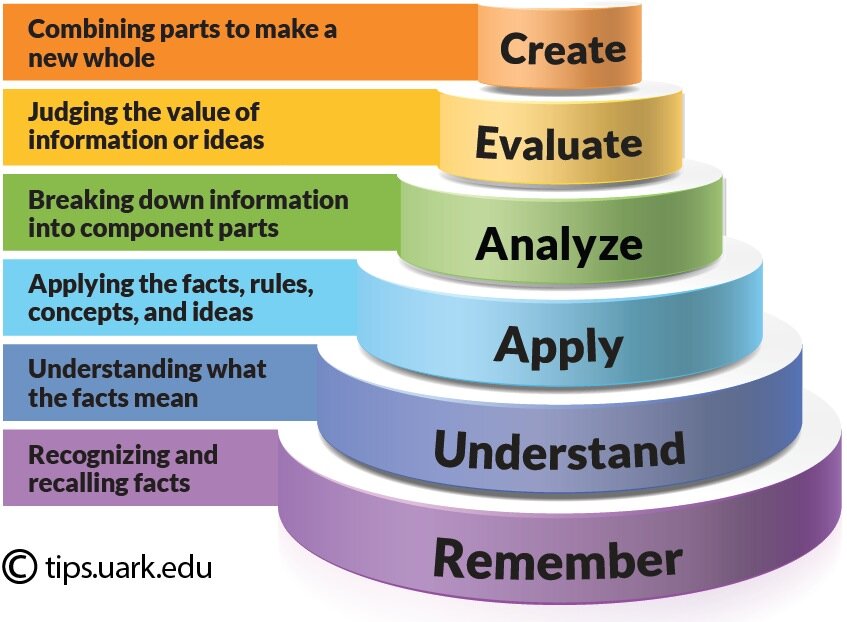
It is not surprising to see that throughout our presentation, it was going to be laid out like Bloom’s Taxonomy Pyramid, see figure 3.
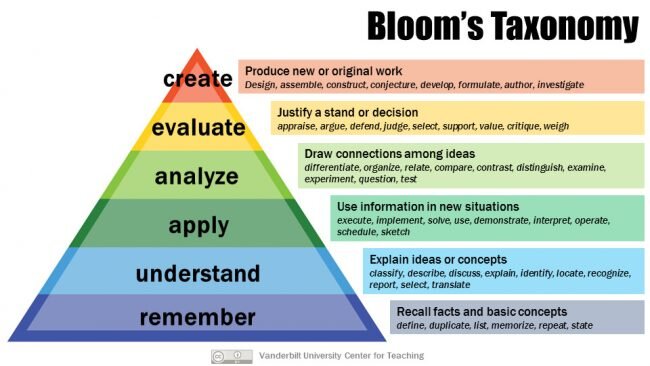
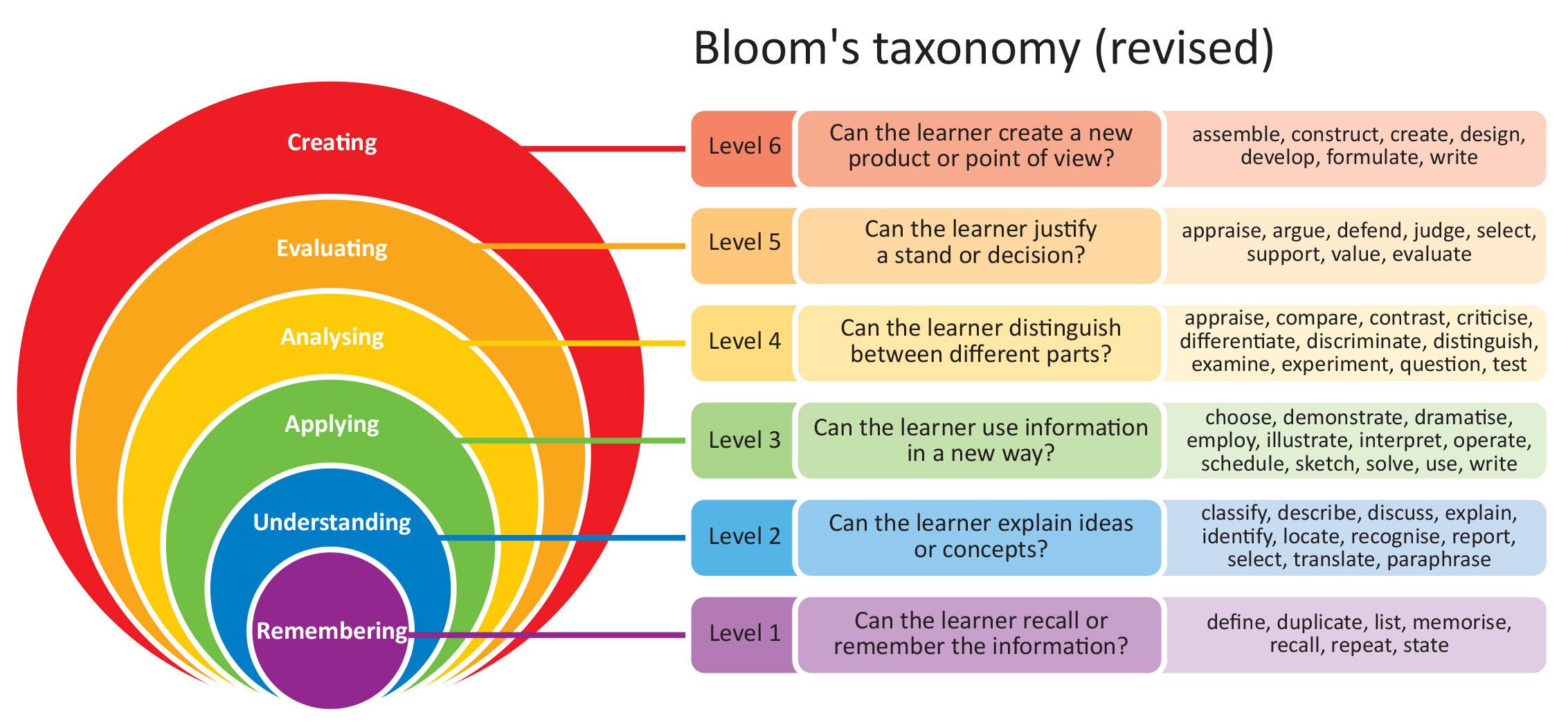
We started with knowledge which represented the surface and passive-like teaching techniques and moved deeper towards evaluation/creation through active learning. Hence, as seen in our lesson plan in table 2 below, at slide 4 we started to move away from lecturing. Slide 4 was a change in our presentation and in its tone/rhythm as it introduces an empty slide with only a heading. The students had to focus on me as I was now using the whiteboard to draw a simple lipoprotein (LPL) with different colours. Upon drawing, I would engage with the students and ask questions about how an LPL would look like or what it would contain. This was an addition from our previous presentation and thought it would be successful in gaining engagement with the students. On Bloom’s Taxonomy Pyramid, we have achieved the middle, which is ‘Apply’. In the Apply section, there is sketching and demonstrating, which was used in slide 4, and interpreting and solving, which was used in slide 5.
Slide 5 introduced ‘show & reveal’, which talked about the different LPL structures, where they are found and what they are predominantly made out of. This technique was utilised for a few reasons as we thought it would 1. engage the students, and 2. recall information that was recently given through a different type of presentation (whiteboard drawings). Slide 6 would also be ‘show & reveal’, however with the addition of a simplified picture-like pathway. Slide 6 was purposefully structured that way to demonstrate a build-on of the ‘show & reveal’ from slide 5. Just how Anthony and Walshaw (2007) in the pedagogy of mathematics, a range of academic outcomes must be available, which includes conceptual understanding, adaptive reasoning and strategic competence. Hence, during our preparation for our presentation, we decided to add a range of activities, learning techniques, different visual cues and simple but solid basics of the overall lesson.
Table 2. A lesson plan that we had to come up with. The lesson plan was very useful in organising our presentation and allowed us to see the big picture.
Slide 7 contained the most challenging concept of our presentation, which is the mode of action (MOA) of statins. We decided to utilise the ‘organizing activities for the students’ technique by Ramsden (2003) as active learning is beneficial and efficient in teaching complicated ideas. This technique puts the focus on the students. The human animation represents the ‘Analyse’ segment on Bloom’s Taxonomy Pyramid where ideas are being connected, visualised, organised and experimented. The human animation had steps in terms of how it would be presented. We came to the conclusion that it would be a good idea to present a general and basic slide of the MOA of statin that also contained a bullet point list.
Whilst performing the human animation, the students could always look back and see where they are at in the MOA. This provided further support. Each student represented a specific part of the MOA of statins and had to act out, on cue, their role. We had to visually think about the 3-dimensional spacing and the number of students involved as we wanted to make sure that each student could see the pathway clearly. We had to think and consider if the MOA of statin was justified for a human animation in the first place as well as which part is important enough to be acted out by a student. Figure 4 below demonstrates a basic sketch of how the students would be positioned for the human animation. We found this method to be useful and effective in organizing ourselves and how we would run the human animation.
Figure 4. Demonstrate how the students were being organized and helped us visualize the 3-dimensional spacing. We wanted to make sure everyone could see everything at any time. Each circle represents a student.
After visualising how the human animation would be, we worked on how it will play out. An introduction to each student and what they represent was made so that everybody knew and understood their role. A description of the scene was next as we had chairs representing a cell membrane with potential receptors. The first run-through of the human animation described the normality of a healthy human body. The second run-through described the pathology of having too much cholesterol in the blood and linked it to slide 3. The third run-through would describe the MOA of statin and how it would reduce low-density cholesterol. The final run-through would be a repeat of how a statin would be applied. We were more comfortable running the human animation in this presentation as we learned from our previous experience. We did this by giving us only 3 minutes to which the human animation was successfully done on time. As the students were going back to their chairs, I would remind them in a quick but efficient fashion about the slide representing the MOA of statin. We believe using the human animation technique with repetition that contained slight variations enhanced the understanding of the MOA of statin concept drastically.
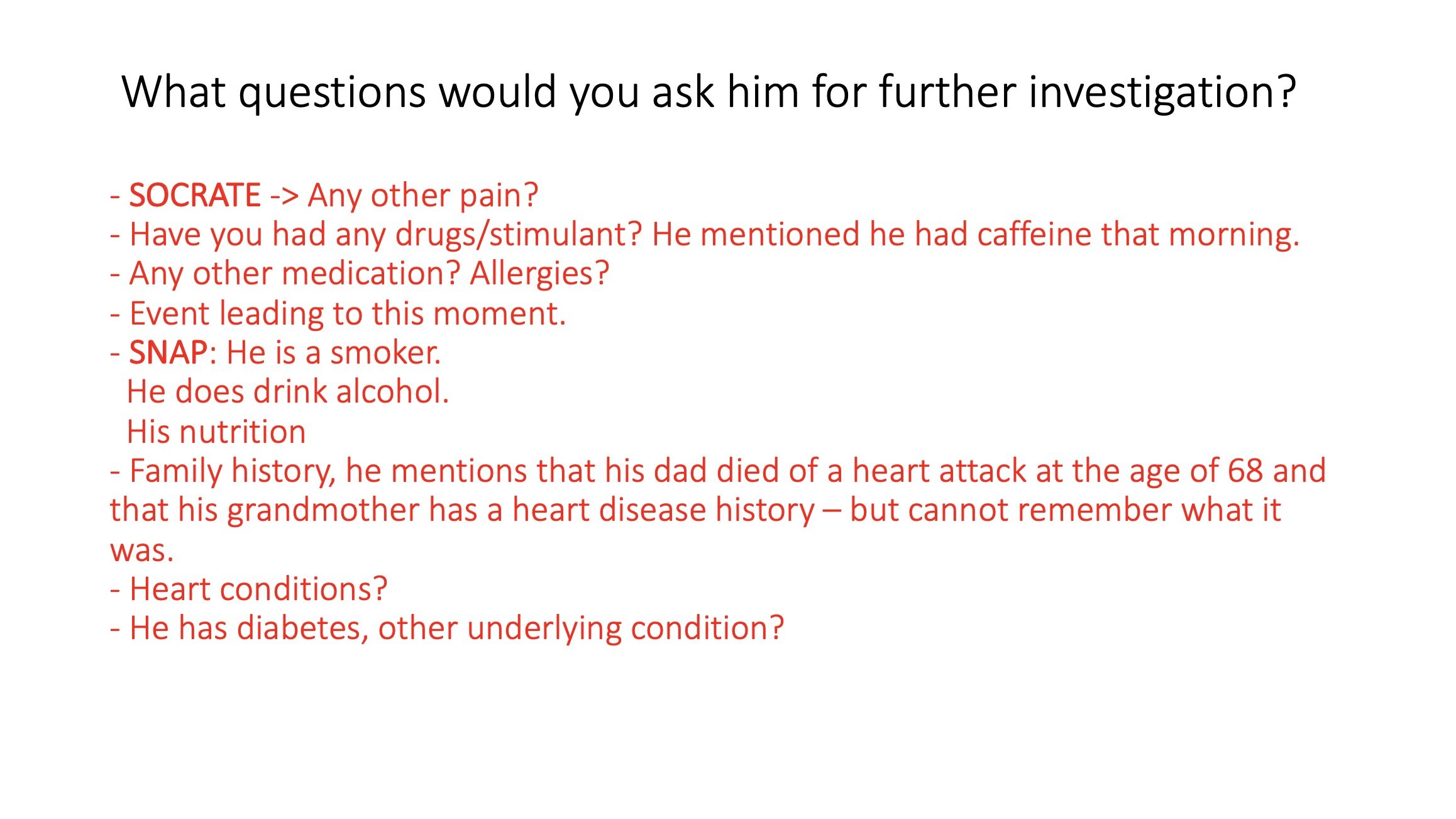
Lastly, to end our presentation with the most effectiveness in education, we decided to produce a case that was incrementally given. However, this time we have added variations as a technique to enhance active learning and utilise the information that has been given to students to critically and justify a pharmacological plan. During the case study, we handed out the risk charts on the wrong side, where the students had to see the other side to calculate the cardiovascular risk with diabetes. This was an added feature from our previous presentation. We also decided to show them the RACGP guidelines to treat dyslipidaemia as it can become complicated when to diagnose or when to start a pharmacological plan. On Bloom’s Taxonomy Pyramid, at this stage of the presentation, we have reached the highest order. This is ‘Evaluation or Create’, which involves judging, developing, formulate, solving and comparing ideas. Finishing with a case study allowed the students to interact fully and critically apply all the information they have received as unbeknownst to them; they were slowly climbing Bloom’s Taxonomy Pyramid during the presentation. We thought this was highly effective in terms of teaching.
We have learned from our previous presentation and through the literature that slight variations and slowly climbing Bloom’s Taxonomy Pyramid were highly effective in transmitting the information. Through the feedback we have been given, we have added the LOs at the end of the presentation to reiterate and enhance all the information we have given to the students. We decided to create exam questions for each LOs and engage with the students to gauge how much they could answer. This allowed us to see if our presentation was successful in terms of teaching and if they were comfortable answering these questions if they were in an exam. This was valuable and immediate feedback as it showed us if we delivered information correctly. When we originally made the LOs that contained the different level of Bloom’s Taxonomy, we asked ourselves if we were confident to answer these questions in an exam after going through our presentation. This was a critical step.
However, we did not manage to reach this section of the presentation as we underestimated how long students take to read a risk chart and answer the case study. We did manage to go through the LOs at the end. We had given ourselves 7 minutes to go through the case with the class, but we still find these estimations hard to be allocated. This resulted in a slight rush and internal panic. Timing throughout a case study is crucial as rushing students will not enable them to grasp the information and think critically. In our future presentations, we shall allow more time in a case study and be more prepared if we are running late or early. However, this is where having experience helps in terms of time management.
ZOOM case study presentation
I had to present, through a ZOOM meeting, a case study. The case study had to run for 20 minutes and had to be adequate and suitable for second-year medical students. This was a valuable and fun experience and there were definitely some challenges such as getting the group’s participation in the case study and how long the case study must be to cover 20 minutes. Overall I received a positive feedback and I was quite proud of my outcome.




Reflecting on how it went
In this extraordinary pandemic time, I had to change my case study delivery so that it would be suitable for a ZOOM meeting. I thus utilised a learning plan and applied what I have learnt along with the pedagogy techniques such as Bloom’s taxonomy to deliver a successful and efficient case study. This is a perfect example when a teacher has to change and modify his/her teaching style due to an unforeseen event. These could be lack of internet, electricity, facility, resources, et cetera. All of these are real examples that I have seen my lecturers go through in South Africa.
The most significant and evident change was going from face to face with a word document case study to online teaching and utilising a PowerPoint case study. The PowerPoint case study was particularly useful and practical as the case study could go section by section while revealing the answers. This technique allowed me to control the pace of the session and ask additional questions that were not officially written down on the case study. I added a photo of myself on the first slide so that the student knew who I was and could put a face to the teacher. This is important for online teaching as learners learn better from teachers who shows whom they are instead of having just the audio. I also accentuated on my voice and tone, avoiding any monotone delivery. The photo was also a backup plan in case the ZOOM video or my computer webcam did not work.
I decided to challenge the students along with basic recalling facts that they should know very well. I used questions that would most likely have an appearance at the end of semester examinations as these are core knowledge. Knowing valuable basics well is the pillar for the addition of fine-tune knowledge. The harder questions were purposeful as I wanted the students to have an open discussion and to promote ‘idea sharing’. I decided to add a relevant clinical aspect to most of the questions as I thoroughly believe that student learns better when they realise the core education they get in the second year is very relevant in clinical settings. I believe this approach was successful as students could think outside the box and use problem-solving skills to come up with a solution together as a group. To promote engagement, I made the student read the case study and questions and ask a different student every time to attempt at answering. This method made everyone feel involved and participating in the case study.
From my experience having gone through case studies, there is nothing more frustrating than getting vague answers. Hence, my answers to my questions were detailed with the addition of pictures to guide the students. I also added questions and answers that were relevant to first-year medicine as I wanted to show the students that first-year basics are beneficial. For example, the basics and importance of history taking and asking questions to a patient. I was nervous with the internet connection as I was on a rural farm which added a lot more pressure on the delivering of the case study. I did mention to give me three minutes if my internet went down and told my students about my situation. Luckily, the internet behaved. The biggest challenge that my colleagues and I could agree on was how long the case study should be. We all presented to each other our case study in a mock practice session by using ZOOM and found that the case would drastically speed up or slow down depending on the interaction between the students. Having a group that does not want to participate or reluctantly want to give answers slows the whole process; however, the opposite can occur. Having a stranger coming into a homegroup that had time to bond with each other can bring some awkwardness and make the group uncomfortable. This was made worst by using distance learning. I had the idea of using an online ice breaker where we would play a short game of Pictionary. I did not use this method as my colleague suggested that I would be running out of time, but it was an exciting idea. In future, I shall research more on online ice breakers. I believe it could make a session even more successful through greater student engagement. In the end, my case study was too long to which I decided to end after my second scenario. I decided to add more content than having not enough scenarios or questions as if it was too long, I could simply end wherever I wanted. The students did want more of my questions; hence I handed in my scenarios to the group facilitator with the answers. This is a valuable feedback as it demonstrates the students wanted more and that the case was relevant to them.
Published 15th March 2020. Last reviewed 1st December 2021.

Reference
Anthony, G., & Walshaw, M. (2007) Effective pedagogy in mathematics. Ministry of Education; Wellington, New Zealand.
Bloom, B.S., Krathwohl, D.R., & Anderson, L.W. (2001) A taxonomy for learning, teaching, and assessing: a revision of Bloom's taxonomy of educational objectives. New York: Longman. https://cft.vanderbilt.edu/guides-sub-pages/blooms-taxonomy/.
Brighton Authors. Assessment & Grading Criteria. University of Brighton website. https://blogs.brighton.ac.uk/askarchitecturedesign/coursework-and-assignments/assessment-grading-criteria/. Updated March, 2012. Accessed February 25, 2020.
Carmichael C, Callingham R, Watson J, Hay I. Factors influencing the development of middle school students' interest in statistical literacy. Statistics Education Research Journal. 2009;8(1):62-81.
https://researchoutput.csu.edu.au/ws/portalfiles/portal/8804244/PID28517postpub.pdf.
Classroom Authors. Factors That Affect Individual Learning. Classroom website. https://classroom.synonym.com/factors-affect-individual-learning-8207913.html. Accessed February 25, 2020.
Chatterjee D, Corral J. How to Write Well-Defined Learning Objectives. J Educ Perioper Med. 2017;19(4): E610. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5944406/.
Colorado University Authors. Guidelines for Writing Learning Objectives. Colorado University School of Medicine website. http://www.ucdenver.edu/academics/colleges/medicalschool/education/degree_programs/MDProgram/administration/curriculumoffice/Documents/CUSOM_Learning-Objectives-Guidelines.pdf. Updated December 1, 2019. Accessed February 27, 2020.
Cornell Authors. Center for Teaching Innovation: Using Rubrics. Cornell University website. https://teaching.cornell.edu/teaching-resources/assessment-evaluation/using-rubrics. Accessed February 25, 2020.
Darlo Authors. Malcolm Knowles’ 6 Adult Learning Principles. Darlo website. https://darlohighereducation.com/news/malcolmknowles6adultlearningprinciples/. Updated November 3, 2016. Accessed February 26, 2020.
Knowles, M. The Adult Learner: A Neglected Species. 3rd ed. Houston: TX Gulf Publishing.
Mubuuke AG, Louw AJN, Schalkwyk SV. Cognitive and Social Factors Influencing Students׳ Response and Utilization of Facilitator Feedback in a Problem Based Learning Context. Health Prof Educ. 2017;3(2):85-98. https://www.sciencedirect.com/science/article/pii/S2452301116300335.
Nilsson, S., Pennbrant, S., Pilhammar, E., & Wenestam, C. (2010, January 28). Pedagogical strategies used in clinical medical education: an observational study. BMC Med Educ, 10(9). 10.1186/1472-6920-10-9.
Ramsden, P. (2003) Learning to teach in higher education (2nd ed.). London: Routledge Falmer.
Shubham D, Biro P. Exploration of Factors Affecting Learners' Motivation in E-learning. IJSRCSEIT. 2019;5. https://www.researchgate.net/publication/336285085_Exploration_of_Factors_Affecting_Learners'_Motivation_in_E-learning.
Surrey Authors. University of Surrey Grade Descriptors: Undergraduate Programmes. University of Surrey website. https://www.surrey.ac.uk/cead/resources/documents/University_of_Surrey_Grade_Descriptors.pdf. Accessed February 25, 2020.
WHO. Hypertension. WHO website. https://www.who.int/news-room/fact-sheets/detail/hypertension. Updated September 13, 2019. Accessed February 19, 2020.
ADDITIONAL SOURCE OF INFORMATION:
Christopher Pappas. The Adult Learning Theory - Andragogy - of Malcolm Knowles. E-learning Industry website. https://elearningindustry.com/the-adult-learning-theory-andragogy-of-malcolm-knowles. Updated May 9, 2013. Accessed February 26, 2020.



